Surgery for childhood brain and spinal cord tumours
Surgery is a medical procedure to examine, remove or repair tissue. Surgery, as a treatment for cancer, means removing the tumour or cancerous tissue from the body.
Surgery is usually used to treat childhood brain and spinal cord tumours. It is commonly the first treatment used. Some tumours may not be treated with surgery alone, but surgery can reduce the amount of tumour that needs to be treated with radiation therapy or chemotherapy. Surgery can also improve the results of these treatments.
Surgery may be used to:
- completely remove a tumour
- remove as much of a tumour as possible before other therapies are given
- do a biopsy of a tumour to confirm the diagnosis of cancer
- relieve symptoms related to the tumour (called palliative surgery)
- insert a plastic tube (shunt) to drain cerebrospinal fluid (CSF) to relieve pressure on the brain
- place a special dome-shaped device (Ommaya reservoir) to remove CSF or give immunotherapy
Sometimes surgery can't be done because the tumour is in part of the brain or spinal cord that is hard to reach or that is too important to risk damaging it when trying to remove the tumour. Tumours that can't be removed are called inoperable or unresectable.
Before surgery
A child with a brain or spinal cord tumour is evaluated very carefully before surgery. A neurological exam will be done to look for any changes to normal functions, such as reflexes, speech, hearing, vision, thinking, movement, feeling and body functions.
Before surgery, doctors may need to give corticosteroids to reduce swelling, relieve symptoms and improve neurological function. Doctors may also give antiseizure or anti-epileptic medicines to control seizures.
The healthcare team will use a CT scan or MRI to carefully map the location of the tumour before surgery. This will help the surgeon decide if the tumour can be removed with surgery. They may also use a functional MRI to plan surgery so that they can avoid important areas of the brain. A functional MRI involves asking the child to answer questions or move certain parts of the body while scans are being done.
Types of surgery
The following types of surgery may be used to treat childhood brain and spinal cord tumours. The type of surgery used will depend on the size and location of the tumour, the type of tumour and the child's age.
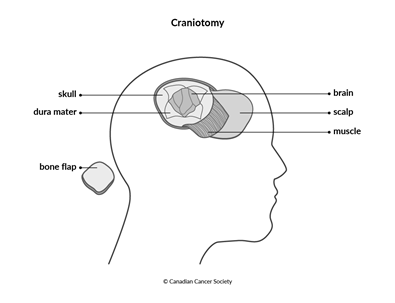
Craniotomy
A craniotomy is the most common type of surgery used to treat brain tumours. The goal of the surgery is to remove as much of the tumour as possible without damaging important brain tissue or affecting brain functions. Image-guided surgery may be used for some brain tumours. This involves taking images with an MRI or a CT scan during the operation to show the location of the tumour and the surgeon’s instruments.
A craniotomy may be done under general anesthesia, but your child may be awake for at least part of the surgery. If the doctor needs to assess brain function (called brain mapping) then your child will need to be awake.
Part of the head may be shaved before surgery. During the surgery, a cut (incision) is made in the scalp. A piece of the skull is removed to expose the area where the brain tumour is growing. This piece of skull is often called the bone flap. The surgeon then makes a cut in the covering of the brain (dura mater) and pulls it apart slightly to find and reach the tumour. The surgeon removes as much of the tumour as possible.
A special ultrasound machine is sometimes used to break up the tumour and make it easier to remove. The surgeon may also use a special operating microscope to help identify the edges of the tumour.
Once the surgeon has removed as much of the tumour as possible, the dura mater is tightly stitched together, the piece of skull is replaced with small screws and plates and the scalp is closed with stitches or staples. If the brain is very swollen after surgery, the piece of skull may be replaced later when the swelling has gone down. Healing usually takes several weeks.
Brain mapping
Brain mapping is done during a craniotomy when a tumour is near areas of the brain that control speech or movement. This lowers the risk of removing or damaging important areas of the brain.
Intra-operative cortical stimulation is used to determine the function of a particular part of the brain. The surgeon stimulates different places on the surface of the brain with a mild electric current. This procedure is painless. It causes a temporary speech disturbance or twitching in the part of the body that is controlled by the area of the brain being stimulated. The healthcare team then "maps" this information so that the surgeon can avoid these areas when removing the tumour. Doctors may also use an MRI or other imaging tests during surgery to show the location of any remaining tumour so that they can remove it safely.
Speech mapping tracks the areas around the tumour that are responsible for talking and understanding speech. After a general anesthetic is given, the surgeon opens the skull and dura mater to expose the brain. The child is then woken up so that they can talk to the surgeon and follow any instructions given during the mapping, such as repeating words or counting. When the mapping is finished, the child is given a general anesthetic again and the surgeon continues the operation to remove the tumour.
Motor mapping tracks the areas around the tumour that are responsible for movement and reflexes. The child may remain under general anesthetic if the surgeon doesn't need their direct feedback. The surgeon stimulates the areas around the tumour with an electrical current and watches for any movement of the body. As with speech mapping, the surgeon uses the mapped areas as a guide when removing the brain tumour.
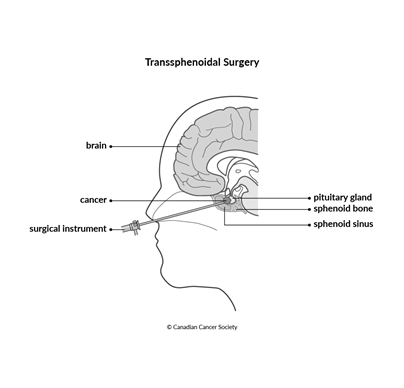
Transsphenoidal surgery
Transsphenoidal means the surgeon goes through the sphenoid sinus to access the tumour. Transsphenoidal surgery may be used to remove some types of brain tumours that are located near the pituitary gland. It is usually only possible for smaller tumours. Larger tumours often need to be removed with a craniotomy.
Transsphenoidal surgery is done under general anesthetic. The child’s head will be placed in a headrest to keep it still during surgery. The surgeon makes a cut under the upper lip along the gum line or at the bottom of the nose between the nostrils. The surgeon then cuts through the sphenoid bone to reach the area around the pituitary gland. The surgeon removes as much of the tumour as possible using special tools. The cut is closed and the nostrils are packed with gauze or a special nasal sponge.
The nostrils will be packed for a few days so your child will need to breathe through the mouth.
Surgery to treat cerebrospinal fluid (CSF) buildup
Brain tumours can block the flow of
This can cause headaches, vomiting, irritability and seizures. In infants, it can also cause a bulging soft spot on the head. Surgery to remove the tumour can help relieve these symptoms, but there are also other ways to drain away excess CSF and lower pressure in the skull.
Placing a shunt
A shunt is a narrow, soft, flexible piece of tubing. It has a valve system that regulates the pressure of the CSF and prevents fluid from flowing back into the chambers of the brain (called ventricles). Many shunts have reservoirs that may be used to remove CSF samples.
During surgery, the shunt is placed in a ventricle of the brain that is filled with CSF. It leads from the ventricle to the scalp. From there, it runs under the skin of the neck and chest and into the abdominal cavity (not the stomach). The CSF that drains into the abdominal cavity is reabsorbed into the bloodstream. Most shunts are permanent.
Placing an external drain
Surgeons use a procedure called a ventriculostomy to place an external ventricular drain (EVD). They insert this thin tube through the skin and skull into a ventricle. The EVD allows CSF to drain from the brain into a collection system or bag outside the body.
An EVD is sometimes used to treat a buildup of CSF before or during surgery to remove a brain tumour. It can’t be left in place permanently. So it is typically removed when it is no longer needed, or it is replaced with a shunt if drainage is still needed.
Endoscopic third ventriculostomy
An endoscopic third ventriculostomy (ETV) is a procedure in which the surgeon makes an opening and places a tube in the third ventricle of the brain to allow CSF to flow around an obstruction. The surgeon uses an endoscope to navigate within the ventricle and create an internal bypass.
An ETV is sometimes used to treat a buildup of CSF in the brain. It can also be used to biopsy or remove tumours in the ventricles of the brain.
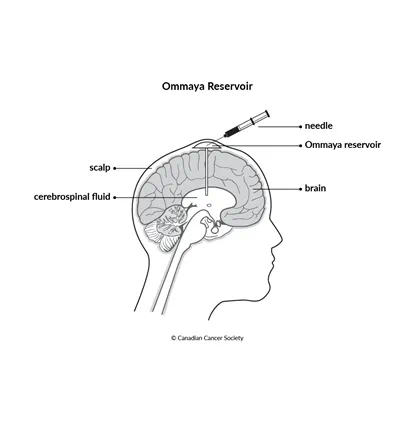
Surgery to place an Ommaya reservoir for drug therapy
An Ommaya reservoir is a small, dome-shaped device with a short tube (catheter) attached to it. The surgeon inserts the reservoir under the scalp, and the catheter is threaded into a ventricle or cyst in the brain.
The reservoir may be used to:
- get samples of CSF
- inject drugs, such as chemotherapy or immunotherapy, directly into the CSF
- inject chemotherapy or immunotherapy drugs directly into a tumour or cyst
- remove extra CSF to relieve pressure
Side effects
Side effects of surgery will depend mainly on the type of surgery and your child's overall health. Tell the healthcare team if your child has side effects that you think are from surgery. The sooner you tell them of any problems, the sooner they can suggest ways to help your child.
Surgery for childhood brain and spinal cord tumours may cause these side effects:
- swelling around the cut (incision)
- infection
- fever
- posterior fossa syndrome
- CSF buildup and leakage
- meningitis
- seizures
- jaw pain
- blood clots
- vision problems
- hormone problems
- behaviour or personality changes
- obesity
Other side effects can develop months or years after treatment for childhood brain and spinal cord tumours. Find out more about late effects of treatments for childhood brain and spinal cord tumours.
Find out more about surgery
Find out more about surgery and the side effects of surgery. To make the decisions that are right for your child, ask the healthcare team questions about surgery.