Bone and muscle problems
Some types of childhood cancer and certain treatments used to treat childhood cancers can have serious effects on bone and muscle growth and development.
How the bones and muscles work
The skeleton is made up of 206 bones. Together, groups of bones of different shapes and sizes form the skeleton. The skeleton gives structure to the body and protects the organs. The bones also make blood cells and store fat and minerals.
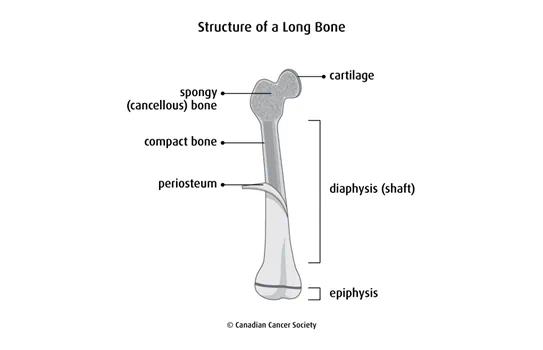
Our body has long, short, flat and irregular bones. The ends of bones are covered by cartilage. Cartilage is a tough, flexible material that is more elastic than bone. It stops the bones from rubbing against each other and lets them move freely at the joints. Long bones are made up of the shaft (called the diaphysis) and the ends (called the epiphyses).
The skeletal muscles are attached to the skeleton and form the flesh of the body. When you contract your muscles, they work with tendons, ligaments and bones to move different parts of your body.
The 2 main types of bone tissue are spongy bone and compact bone. Compact bone is the dense, hard, smooth outer layer of bone. Spongy bone stores red bone marrow where blood cells are made.
Bone has lots of blood vessels. Blood carries oxygen and nutrients to bone cells, which are needed to keep bone tissue healthy. Bones are covered with a layer of periosteum. In a young child, the periosteum also contains many small blood vessels.
Types of bone and muscle problems
Bone and muscle problems that can develop after treatment for childhood cancer include underdeveloped muscles, decreased bone growth, uneven bone and muscle growth, and short height (stature). The bone may grow again but short height can be permanent.
Bone problems that can develop after treatment for childhood cancer include:
- thin or weak bones that can easily break (osteoporosis)
- rounding of the spine (kyphosis)
- curving of the spine (scoliosis)
- bone death(osteonecrosis)
Causes
Some cancers and cancer treatments during childhood can affect the development of bones, joints and muscles.
Type of cancer
Bone and muscle problems can develop as late effects of treatment for some childhood cancers, including brain or spinal cord cancers (central nervous system tumours) and bone cancer (Ewing sarcoma or osteosarcoma).
Radiation therapy
Radiation therapy is the main risk factor for bone, joint and muscle problems. Radiation therapy can slow the growth of bones, soft tissue, muscle and blood vessels when a child is growing quickly. Factors that add to the effect of radiation on developing bones and muscles include:
- age (children younger than 6 or children growing quickly during puberty)
- high doses of radiation
- the size of area treated
- the area of the body treated
Radiation to the abdomen has a risk for scoliosis and underdeveloped muscles in the area.
Radiation to the spine has a risk for shorter overall height or shorter sitting height.
Radiation to the chest or neck has a risk for narrow shoulders, a poorly developed chest or a narrow neck.
Radiation to the hips or long bones in the arms or legs has a risk for arms or legs being different lengths.
Radiation to the central nervous system (brain and spinal cord) has a risk for growth hormone deficiency that can result in short height and changes to the face or skull.
Other factors
Other factors that may increase the risk of bone, joint and muscle problems as a late effect of cancer treatment include:
- being female
- low levels of male or female hormones or growth hormone
- high levels of thyroid hormone
- treatment with corticosteroids, such as dexamethasone (Decadron, Dexasone) and prednisone
- treatment with a stem cell transplant
- treatment with certain chemotherapy drugs, such as methotrexate, cyclophosphamide (Procytox), and ifosfamide (Ifex)
- surgery for cancers that start in the bone or muscle
Symptoms
Signs and symptoms of bone and muscle problems include:
- bone or joint pain
- less range of motion
- joint stiffness
- swelling, redness or warmth over a bone or joint
- sideways turning of the spine
- a hump on the back
- bones that break easily
- being shorter than normal
- unequal growth – the treated side of the body grows differently than the untreated side, so one side of the body looks higher than the other side
- changes in how a child walks
- a body that tilts to one side
- a slouching position when standing or sitting
- less calcium in the bones
If symptoms get worse or don’t go away, report them to your doctor or healthcare team without waiting for your next scheduled appointment.
Diagnosis
Tests to diagnose bone and muscle problems include:
- a physical exam
- an x-ray
- a bone density scan
- an MRI
- a CT scan
- a bone scan
Find out more about these tests and procedures.
Preventing and managing bone and muscle problems
It is important to tell your doctor or healthcare team if you notice any symptoms or a change in symptoms. The goals of treatment for bone and muscle problems are to:
- improve use of the affected bone, limb or joint
- reduce pain
- stop bone and joint damage
Abnormal growth
The healthcare team can recommend special shoes or braces if your legs are different lengths. In some cases, surgery may be used to correct this problem. If there isn’t enough growth hormone and the child doesn’t grow as expected, replacement growth hormones may be given.
Osteoporosis
The following may help to lower your risk of osteoporosis:
- weight-bearing exercises such as brisk walking, dancing and jogging
- higher-impact, weight-bearing activities such as hopping, jogging and jumping rope
- resistance exercises such as light weightlifting
- a diet high in calcium and vitamin D
Medicines can be used to help reduce bone loss and prevent breaks (fractures). The doctor will consider your medical history and the medicines you’re taking when discussing drug treatment for osteoporosis.
Find out more about osteoporosis.
Kyphosis and scoliosis
Kyphosis and scoliosis are usually treated in stages. The first stage involves watching the curve, especially during times of rapid growth (such as puberty). If the curve doesn’t get worse, you may not need any further treatment. If the curve gets worse, you may be given a plastic body brace that is worn under your clothes. The goal of bracing is to prevent further curving or help correct the curve. If the curve is severe, surgery may be needed.
Osteonecrosis
Osteonecrosis most often affects areas of bone around the knees and hips. When deciding the best treatment, the doctor will consider the child’s age, the stage of the osteonecrosis, the location and amount of bone that is affected, the stage and the type of cancer treatment.
Treatment of osteonecrosis may include:
- medicine to reduce pain
- reducing weight-bearing activity, such as by using crutches, to slow damage and promote natural healing
- physical therapy
- electrical stimulation to promote bone growth
- surgery to remove or reposition a weak area of bone, a bone graft, or placing an artificial joint to replace the bone in a joint
You can help reduce further osteonecrosis and cope with symptoms by doing the following:
- Try activities that are good for joint problems, such as swimming and bicycling.
- Avoid activities that put a lot of stress on the joints, such as running and jumping.
- Rest your joints when they hurt.
- Take pain or anti-inflammatory medicines as prescribed by your doctor.
- Follow exercise guidelines given to you by your healthcare team or physical therapist.
Follow-up
All people who are treated for cancer during childhood need regular follow-up. The healthcare team will develop a follow-up plan based on the type of cancer, how it was treated and your needs.
Make sure you tell your doctor all the treatments you received. Follow-up tests may be every 6 months during adolescent growth. If you are at risk for bone and muscle problems, you should have a physical exam each year.
Follow-up tests may include:
- a bone density scan
- a CT scan
- x-rays
Your trusted source for accurate cancer information
With support from readers like you, we can continue to provide the highest quality cancer information for over 100 types of cancer.
We’re here to ensure easy access to accurate cancer information for you and the millions of people who visit this website every year. But we can’t do it alone.
Every donation helps fund reliable cancer information, compassionate support services and the most promising research. Please give today because every contribution counts. Thank you.