Surgery for non–small cell lung cancer
Surgery is sometimes used to treat lung cancer. It is used more often for non–small cell lung cancer than for small cell lung cancer. The type of surgery you have depends mainly on the size of the tumour, where it is and how far it has spread within the lung. When planning surgery, your healthcare team will also consider other factors, such as your age, overall health and how well your lungs are working.
Surgery may be done for different reasons. You may have surgery to:
completely remove the tumour
reduce pain or ease symptoms (called palliative surgery)
Evaluation for surgery
Before surgery is offered as a treatment for lung cancer, your healthcare team must decide if the cancer can be removed with surgery.
Diagnostic tests are used to find out the size of the tumour and where the cancer has spread. These tests can help your healthcare team decide if surgery can be done.
Unresectable means that the cancer cannot be completely removed with surgery. Some things that make a tumour unresectable include the following:
- A tumour is too large to be removed or is in a place in the body where it can't be completely removed.
- The cancer has spread to lymph nodes near the collarbone, to lymph nodes in the middle of the chest on the opposite side from the tumour, or to lymph nodes where the windpipe (trachea) splits into the 2 bronchi on the opposite side from the lung tumour.
- The cancer has spread to other organs near the lungs or to other parts of the body.
- There is fluid around the lungs (pleural effusion) or around the heart (pericardial effusion).
Resectable means that the cancer can be completely removed with surgery.
If the cancer is resectable, your healthcare team will look at your lung and heart function test results to see if you are healthy enough to have surgery for lung cancer. You need to be in good overall health and need to have enough lung function after surgery. Surgery is offered mainly to people who have a low risk of developing shortness of breath and other lung problems after surgery. If you are at a higher risk of poor lung function and shortness of breath, your healthcare team will talk to you about the side effects of surgery and your quality of life after surgery. Together you will decide what is right for you.
Unfortunately, most people with lung cancer are not in good health and have other serious medical conditions. If you are not well enough to have surgery, your healthcare team will not offer it to you as a treatment option.
Getting ready for surgery
Lung surgery is a major operation. It can be very difficult to recover from it, so your healthcare team will try to make sure you are as healthy as possible before surgery.
If you smoke, it's important that you quit before having surgery. People who smoke are more likely to have heart and lung problems after surgery. Research shows that people who quit smoking before lung cancer surgery have a better chance of living longer and have a lower risk of developing another cancer.
Your healthcare team may also give you an exercise program to do before and after surgery. These exercises help improve deep breathing, coughing and lung capacity. Doing them helps you recover from lung surgery.
Surgeries for non–small cell lung cancer
Lung surgery can be done in 2 ways.
A thoracotomy is the most common way of doing lung surgery. It is done through a cut (incision) in between the ribs on the side of the chest. The ribs are spread apart so the surgeon can reach the lung.
Video-assisted thoracic surgery (VATS) is a less invasive way of doing surgery. A small video camera and surgical tools are inserted through several small cuts in the chest. The surgeon is guided by an image on a video screen. VATS may be used to remove small tumours (tumours that are 3 to 4 cm) that are found on the outer edges of the lung. It may also be used to remove part of a lung.
The following types of surgery are used to treat lung cancer. You may also have other treatments before or after surgery.
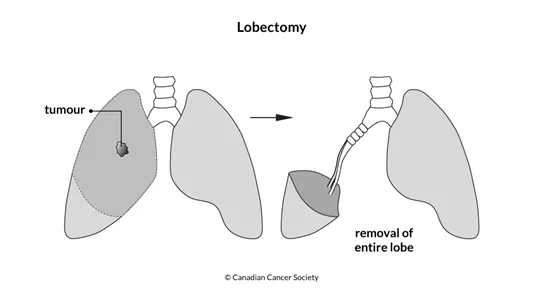
Lobectomy
A lobectomy removes the lobe of the lung where the tumour is.
A bilobectomy removes 2 of the 3 lobes of the right lung. It is a type of lobectomy. This surgery may be done if the tumour has spread to 2 lobes next to each other. The upper and middle lobes or the middle and lower lobes may be removed during a bilobectomy.
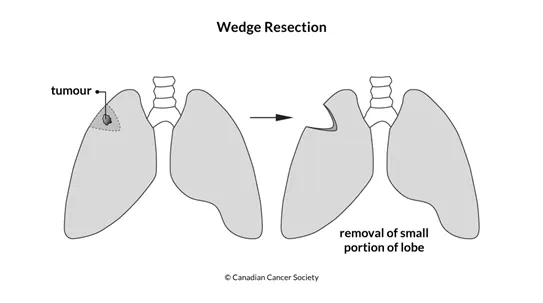
Wedge or segmental resection
A wedge resection removes the tumour along with a margin of healthy tissue around the tumour. A segmental resection removes a wider margin of healthy tissue around the tumour. These surgeries may be offered for very early stage lung cancer to preserve as much lung function as possible. They may also be done in people with more advanced lung cancer who don't have enough lung function to have more of the lung removed.
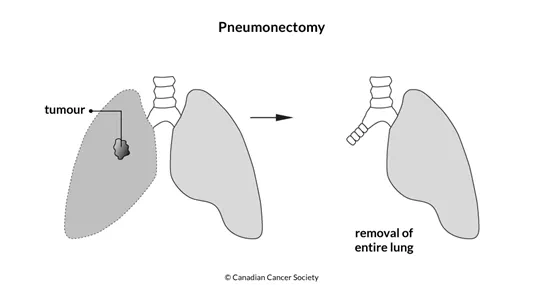
Pneumonectomy
A pneumonectomy removes the whole lung. This surgery is done if the tumour involves more than one lobe of the lung, the tumour is near where the airway tube enters the lung or if there is cancer in the hilar lymph node. It is only done if a lobectomy would not remove all of the cancer.
Recovering from a pneumonectomy is very difficult. Because the right lung is larger, there are more side effects when it is removed.
Extended pulmonary resection
An extended pulmonary resection removes the muscles, nerves, blood vessels and other tissues near the lung. During the surgery, a wide area of tissue surrounding the lung is taken out to remove as much of the cancer as possible.
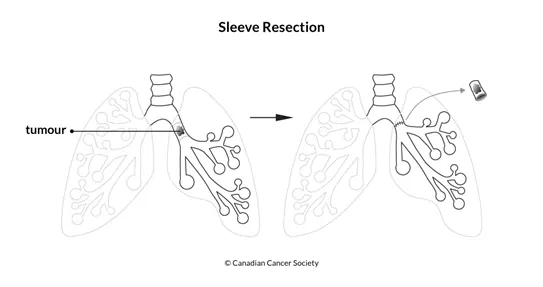
Sleeve resection
A sleeve resection removes the tumour and a margin of healthy tissue on either side of the tumour when the tumour is in one of the lung's airway tubes (the bronchi). The 2 ends of the tube are then joined back together.
Chest wall resection
A chest wall resection removes the muscles, bones and other tissues of the chest wall. It may be done for a superior sulcus (Pancoast) tumour that spreads from the area at the top of the lung into the chest wall. If a large area has to be removed, the surgeon will reconstruct the area during surgery. To reconstruct the area, a special material that moves with the body during breathing is used.
Lymph node removal
Lymph nodes on the same side of the body as the tumour are removed during lung cancer surgery and then checked for cancer.
Sometimes just a few lymph nodes are removed to look for cancer (this is called sampling), but other times all of the lymph nodes are removed.
Surgery for metastasis
If you have lung cancer that has spread to the adrenal gland or to the brain, you may have surgery to remove the metastasis. If lung cancer has spread to the brain, surgery will be a treatment option if there is one tumour only to remove.
After surgery
After lung cancer surgery, you will have a tube or tubes coming out of your chest. These tubes are attached to a canister and they drain extra fluid or air from your chest. They are removed when the air or fluid has stopped draining.
Your healthcare team will encourage you to do the same deep breathing and coughing exercises you did before surgery. Sometimes this can be very hard to do because of the pain after lung cancer surgery. But doing them is an important part of recovery. You will also be encouraged to get out of bed and walk as much as you can.
Side effects
Side effects can happen with any type of treatment for lung cancer, but everyone's experience is different. Some people have many side effects. Other people have only a few side effects.
If you develop side effects, they can happen any time during, immediately after or a few days or weeks after surgery. Sometimes late side effects develop months or years after surgery. Most side effects will go away on their own or can be treated, but some may last a long time or become permanent.
Side effects of surgery will depend mainly on the type of surgery, whether you smoke and your overall health.
Surgery for lung cancer may cause these side effects:
- pain
- cough
- difficulty breathing
- bronchopleural fistula – an abnormal opening between the pleural space and an airway tube of the lung
- collapsed lung
- heart problems
- fatigue
- blood clots
Tell your healthcare team if you have these side effects or others you think might be from surgery. The sooner you tell them of any problems, the sooner they can suggest ways to help you deal with them.
Questions to ask about surgery
Find out more about surgery and side effects of surgery. To make the decisions that are right for you, ask your healthcare team questions about surgery.